条文本

数据来自Altmetric.com
脑炎很少以麻痹麻痹为首发症状。在这里,我们报告一例类固醇反应性双侧额叶皮质脑炎,累及腿部运动区,患者入院时表现为躯体麻痹。有趣的是,最初的残缺症演变为急性播散性脑脊髓炎(ADEM)样疾病和视神经炎,患者被发现抗髓磷脂少突胶质细胞糖蛋白(MOG)抗体阳性。
病例报告
一名46岁男性在2008年9月初经历过短暂性头晕。回顾性脑MRI显示轻微液体衰减反转恢复(FLAIR)高强度病变,累及左额叶皮层(图1).一周后,患者右腿出现局灶性运动性癫痫,随后扩散。此后,患者在一周内逐渐出现头痛和肢体麻痹。入院时,患者表现为无其他神经功能缺损的麻痹,但脊柱MRI检查正常。脑电图显示没有癫痫性放电。脑脊液(CSF)检查显示白细胞升高(56 /µL;93%单个核细胞,3%多形核白细胞)和正常蛋白质(36 mg/dL)和葡萄糖(59 mg/dL)水平。脑脊液中的髓鞘碱性蛋白(MBP)和胶质纤维酸性蛋白水平未升高。脑脊液中抗n -甲基- d-天冬氨酸受体(NMDAR)抗体、抗电压门控钾通道(VGKC)抗体、抗-氨基-3-羟基-5-甲基-4-异恶唑丙酸受体(AMPAR)抗体和抗-γ-氨基丁酸-B受体(GABA(B)R)抗体的细胞检测均为阴性。传染性中枢神经系统(CNS)疾病、胶原蛋白疾病、血管炎、Behçet病、结节病、淋巴瘤、副肿瘤综合征、维生素B缺乏症和桥本脑病的血液和脑脊液检查无显著性差异。

{kind=link}
{kind=link}
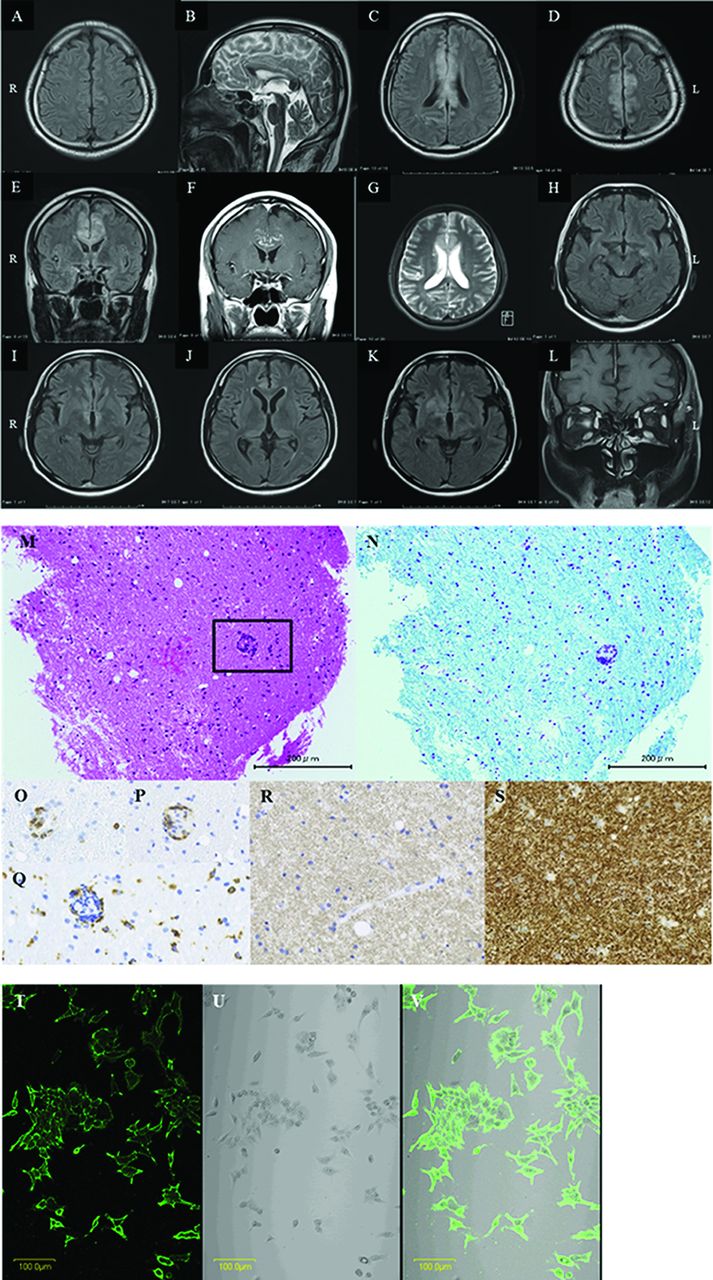
上面板:轴向流体衰减反演恢复(FLAIR)图像(1.5 T;TR 6000 ms, TE 105 ms)。(A)发病时MRI显示左额叶皮层有微弱高强度病变,DWI显示正常。矢状t2加权图像(1.5 T;TR 3210 ms, TE 105 ms) (B)和轴向和冠状位FLAIR图像(C-E)。入院后12天MRI示胼胝体、双侧扣带回及双侧额叶内侧高强度病变,DWI表现为微弱高强度区。冠状面t1加权图像(1.5 T;增强后TR 470 ms, TE 15 ms) (F)。脑MRI显示这些病灶增强,类固醇脉冲治疗后减弱。轴向t2加权图像(1.5 T;脑活检前TR 3200 ms, TE 544 ms) (G)显示包括扣带回、胼胝体和双侧额叶内侧的高强度信号。 Axial FLAIR images from November 2008 (H–J) revealed new high-intensity lesions surrounding the third ventricle and aqueduct of the midbrain and in the bilateral thalamus, although the high-intensity lesions involving the corpus callosum, bilateral cingulate gyrus and medial side of the bilateral frontal lobes had been resolved. Axial FLAIR images from January 2009 (K) revealed a new high-intensity lesion in the right basal ganglia. Coronal T1-weighted image (1.5 T; TR 615 ms, TE 15 ms) with gadolinium enhancement from August 2010 (L) revealed the enhancement of the right optic nerve. Middle panel: Paraffin-embedded biopsied brain slices. (M) The tissues were extensively spongy, reflecting brain oedema. Some cerebral vessels (rectangle) were cuffed with inflammatory cells. (H&E stain; 200x.) (N) Myelin sheaths throughout the biopsy samples were densely stained with luxol fast blue, thus indicating no evidence of demyelination (Kluver-Barrera stain; 200x). (O–Q) Perivascular cuffing shown in M. T and B lymphocytes infiltrated around the vessels, whereas macrophages were more diffusely scattered in the brain parenchyma (O, CD3; P, CD20; Q, CD68; 400x). (R) The immunostaining of myelin oligodendrocyte glycoprotein (MOG) also revealed intact myelin sheaths (MOG; 400x). (S) Axons stained for neurofilaments were quite well preserved. Only a few axonal alterations were observed in the sample. Lower panel: Indirect immunofluorescence assay of live human-MOG-transfected cells stained with the serum of the patient. MOG cDNA is expressed on the cell surface. (T) HEK293 cells transfected with MOG were stained with the serum of the patient and fluorescein-conjugated goat anti-human IgG antibody. (U) Bright-field micrograph of the cells. (V) Merge of T and U. The cell surface was stained positive.
入院后,截瘫逐渐进展,患者在入院后12天完全截瘫伴痉挛。出现发热、记忆力下降、嗜睡等症状。大脑it2加权和FLAIR MRI显示胼胝体、双侧扣带回和双侧额叶内侧高强度增强(图1B-F)。我们怀疑是某种类型的脑炎,因此开始大剂量静脉注射甲泼尼龙(1 g, 3天)和阿昔洛韦(1500 mg/天)。他的症状随后得到改善,并于2008年10月初开始口服泼尼松龙(PSL) (60 mg/天)。当时,脑脊液检查显示寡克隆IgG条带阳性,后来在2008年10月中旬变为阴性。在2008年10月初重新评估时,CSF-MBP没有升高。
由于诊断的不确定性,于2008年11月初在右侧扣带回进行了脑活检。病理检查显示组织损伤相对较轻,无脱髓鞘斑块,神经元或轴突损失或星形细胞破坏,尽管有t细胞和b细胞浸润的炎症和水肿改变。未观察到肿瘤细胞(图1m)。症状明显改善,所以PSL逐渐减少到20mg /天。
2008年11月下旬,虽然原有FLAIR高灶区变小,但在第三脑室和大脑导水管周围、双侧丘脑和右基底核出现新的无症状FLAIR高灶。然而,这些病变后来自发消退(图1H-K)。PSL逐渐减少至7 mg/d。2009年3月,患者可自主行走,出院。此时,原有FLAIR高强度区也明显变小。
2010年7月下旬,PSL从5毫克/天进一步减少到4毫克/天。1个月后,患者右侧视神经炎复发(图1L).他右眼视力为20/200。他抗血清水通道蛋白4抗体呈阴性。脑脊液检查显示白细胞正常值(1 /µl;100%单核细胞),蛋白质(29.6 mg/dL)和葡萄糖(55 mg/dL)。病人接受了类固醇治疗,结果完全康复。此后,继续给予PSL (5mg /天)。他最终的库尔茨克残疾状况扩展量表为2.0。
2014年2月,我们的室内细胞基础检测1显示患者血清抗mog抗体阳性(图1过程)。他在2008年10月中旬脑炎首发期间、2010年8月下旬视神经炎复发期间和2014年2月下旬缓解期间的抗体滴度分别为4096倍、4096倍和512x。
讨论
我们的病例是独特的,患者脑炎累及双侧额叶皮质区,入院时表现为脑残。急性和亚急性非创伤性截瘫的常见原因是胸脊髓的炎症性、血管性和肿瘤性疾病,但也有一些罕见的非脊髓性原因的截瘫,如多神经根炎、高钾性或低钾性瘫痪、心源性截瘫和旁矢状面皮质综合征。2虽然在大脑前动脉区域双侧缺血和旁矢状动脉区域快速生长的肿瘤的病例中可以观察到双侧旁矢状动脉皮质综合征,但脑炎通常不包括在截瘫的鉴别诊断中。2
本病例在诊断脑炎、adm样病变和单侧视神经炎时抗mog抗体阳性。我们认为抗mog抗体参与了本病例的adem样病变和视神经炎,因为其临床病程和MRI表现与报道的抗mog抗体阳性病例相似。然而,抗mog抗体在独特的脑炎中的发病机制尚不清楚,因为先前在抗mog抗体阳性的患者中既没有显示脑活检中的脱髓鞘病变,也没有显示CSF中MBP水平升高3 4在本案中得到证实。最近,抗nmdar脑炎和抗mog抗体相关脱髓鞘综合征并存的病例已被报道。5在我们的病例中,虽然未检测到NMDAR、VGKC、AMPAR或GABA(B)R抗体,但涉及这些抗体的自身抗体介导的脑炎以外的自身免疫性脑炎可能与抗mog抗体相关的脱髓鞘综合征共存。需要进一步的研究来阐明抗mog抗体相关疾病的扩展谱。